Arthritis after cancer immunotherapy:
F18-FDG PET/CT imaging

Figure 1: Maximal intensity projection (mip) image, showing increased FDG uptake around the right shoulder and left knee (red arrows).
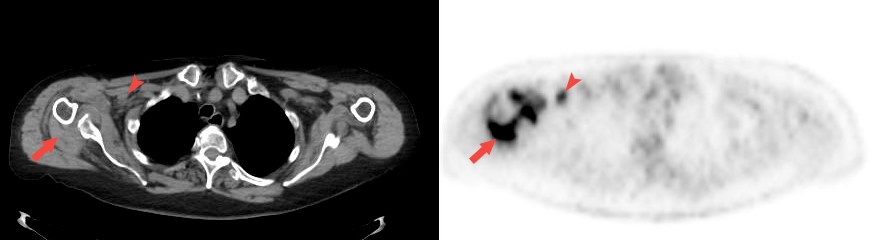
Figure 2: Trans-axial image (CT left; PET right) showing increased uptake around the right shoulder as well as increased uptake in an axillary lymph node.
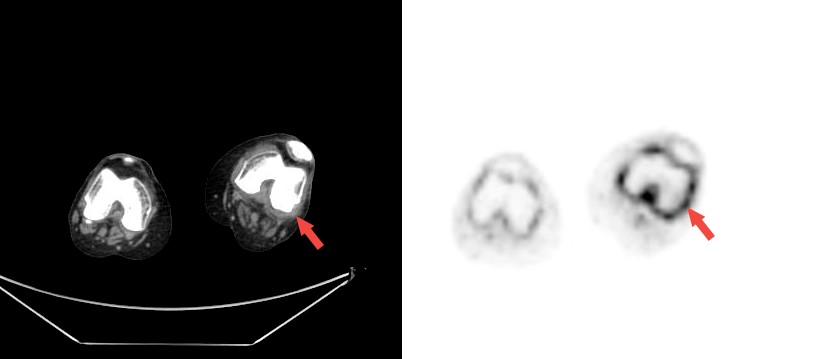
Figure 3: Trans-axial image (CT left; PET right) showing increased uptake around the left knee.
Description:
A 78 y/o female with metastatic melanoma underwent an F18-FDG PET/CT scan as part of routine follow-up during therapy with Opdivo (Nivolumab) an anti-PD1 antibody (programmed cell death protein 1).
The PET/CT scan showed no clear evidence of active malignancy; however, intense diffuse uptake was evident in the synovium of her left knee as well as her right shoulder, thought to represent arthritis of large joints, perhaps secondary to treatment with immunotherapy. Increased uptake was also noted in two small right axillary lymph nodes, assumed to be reactive to the synovitis in the ipsilateral shoulder.
The patient had a full rheumatologic evaluation, including complete blood work that was negative for any rheumatologic markers, and drainage of synovial fluid from affected joints, which was consistent with inflammation without any signs of infection or crystal deposition. A diagnosis of seronegative polyarthritis secondary to treatment with Opdivo was made.
Discussion:
Checkpoint inhibitor immunotherapy has become standard of care in metastatic melanoma and its use is also increasing in other cancers. As an activator of the immune system, this class of drugs has the potential to cause inflammatory side-effects in different organs, most commonly endocrinopathies, colitis, dermatitis, hepatitis, and pneumonitis. Arthritis is also a potential inflammatory side-effect, although much less common. The present case illustrates the importance of PET/CT in patients receiving immunotherapy, not only in evaluating response to therapy and disease status, but also as a whole body imaging modality able to detect and monitor inflammatory side-effects in different systems.
References:
- Smith MH, Bass AR, Arthritis after cancer immunotherapy: symptom duration and treatment response.Arthritis Care Res (Hoboken). 2017. doi: 10.1002/acr.23467. [Epub ahead of print]
- Cappelli LC, Shah AA, Bingham CO 3rd. Immune-Related Adverse Effects of Cancer Immunotherapy— Implications for Rheumatology. Rheum Dis Clin North Am. 2017; 43:65-78.
This Case was kindly provided by:
Dr. Jonathan Kuten MD MHA
Dept. of Nuclear Medicine, Tel Aviv Sourasky Medical Center,
6 Weizmann St., Tel Aviv, 4263906 Israel
Tel: +972-3-6973536, FAX: +972-3-6973895
Contact
Prof. Einat Even-Sapir MD, Phd
Head, Dept of Nuclear Medicine, Tel Aviv Sourasky Medical Center, Tel Aviv University
More cases

Case No. 22
Primary intestinal diffuse large B-cell lymphoma (DLBCL)
Case No. 21
Primary carcinoid tumor of the lung
Case No. 20
Takayasu arteritis: 18F-FDG-PET/CT